
Choices from the 40th week of your pregnancy
Overdue babies
If a baby is born after 42 weeks it is called a ‘post term’ baby. The Dutch medical term for overdue pregnancies is serotinity. We speak of imminent serotinity as from the 41st week of pregnancy and of serotinity from the 42nd week. When both baby and mother are in good health there are no medical reasons for inducing the birth. Various choices, such as waiting, stripping the membranes or inducing labour are completely up to yourself and your partner. In this brochure you will find more information describing these choices.
The due date
The due date is calculated in the first weeks of a pregnancy. 40 weeks (280 days) are counted as from the first day of your last period. This calculation is then more accurately pinpointed during the dating ultrasound scan.
Not many women give birth on the calculated due date. In fact, only 3 – 5% will. Labour usually takes place between 37 and 42 weeks. This is the period of term expected in a normal pregnancy. Approximately 10% of all pregnancies last longer than 41 weeks.
Should you give birth before 37 weeks, this is considered a premature birth. If you give birth two weeks after the calculated due date, the birth is considered overdue. You will then have been pregnant for 42 weeks. After 42 weeks there is medical reason to induce labour. You will then need to give birth in a hospital under the supervision of a gynaecologist.
We know that placenta function tends to taper off during the end of a pregnancy; it may not supply all of the baby’s needs. The amount of amniotic fluid can also reduce. The risk of faeces (meconium) coming from the baby and into the amniotic fluid increases after the calculated due date. We don’t exactly know whether and when this will happen. We do know that it is important to check up the baby’s movements and when in doubt this check up should take place at hospital. By taking a cardiotocogram (CTG) the baby’s condition can be assessed. A CTG measures the baby’s heart rate for about 30 minutes. An ultrasound scan is also done to calculate whether there is sufficient amniotic fluid available.
1st choide: Wait
If all of the check ups go well and the pregnancy is medically considered to be a healthy one it is best to wait until the end of the calculated due date period (up to the full 42 weeks) for a spontaneous labour. What is most important is that both you and the baby feel good, and that you can feel the baby move just like you have in the preceding weeks.
When you wait you are giving your body all the time necessary to allow the natural process to mature. Once mature, your body will be ready to give birth and you will not need to push with as much force. On top of this, natural labour usually goes much more smoothly and easily. Most women remember the experience in a more positive way if labour has been experienced under natural circumstances.
If you choose to wait until 42 weeks, the midwife will assess the amniotic fluid supply via ultrasound as from week 41 or thereabouts. In order to keep track of your pregnancy you will undergo twice weekly check ups from 40 weeks. If you are still pregnant and coming up to 42 weeks, you may choose a hospital and we will arrange for you to be assessed there as from 41 weeks and 5 days. A hospital will evaluate the condition of the baby by means of an ultrasound and cardiotocography (CTG). We will then know whether there is sufficient amniotic fluid, and also how big the baby is. Furthermore, an internal exam will be carried out to see whether the cervix is ready for the birth. It is very important that you continue to feel the baby move energetically. After these tests it is up to you whether to induce labour or not. But should the baby be less lively, the amniotic fluid judged to be too little or not at an optimal level, and the CTG does not optimal results, necessary actions will be taken relatively quickly.
Stripping of the membranes
One way to speed up labour is to stimulate the uterus. The midwife does this by ‘stripping’ the membranes from the cervix wall. This can be done from the calculated due date (40 weeks). Membranes ‘stuck’ to the inside of the cervix wall are loosened during an internal exam. By stripping them out, the hormones that encourage cervix dilation are released, which can act as a catalyst for labour. The membranes remain intact and are not actually broken. Stripping gives no additional complications. Before stripping can be started an internal exam is carried out to assess cervix maturity. Your cervix should be flexible, slack and a little open before stripping can be done. This is more common if you have previously given birth. Stripping is not possible in a rigid, closed cervix.
Stripping during an internal exam is not a particularly pleasant experience. You can always let us know if you are too uncomfortable, in which case we can stop. After an internal exam or stripping a little blood loss may occur. Sometimes blood is accompanied by mucus, or a loosening of the mucus plug. This is a totally normal phenomenon; the blood comes from the richly network of blood vessels which run throughout the cervix, and not from your baby so you don’t need to worry. For many, this blood loss is like the worst day of a period. If you feel like you are losing more than this, you should call for us. Stripping can also often lead to period pain-like cramps. These encourage the initiation of your labour.
Our ultimate goal is that these cramps turn into contractions. You will notice that the cramps become more painful, as well as more regular and with shorter breaks between them. If this does not happen after the stripping procedure, it can be repeated. We can perform stripping during your twice weekly check ups.
2nd choice: Induces labour
In Rotterdam you can choose to induce labour as from 41 weeks. Induction is the artificial initiation of your labour. This is done with drugs which induce contractions. The artificial stripping of membranes can contribute to this. Induced labour always takes place in hospital, and under the supervision of a gynaecologist.
Hospital check ups
If you choose to induce labour from 41 weeks, we will make you an appointment at the hospital at 40 + 5 days for a check-up. This does not mean you will be induced straight away. First an ultrasound and CTG will assess the baby’s condition and size, and make sure there is sufficient amniotic fluid. An internal exam will also be carried out to see at what stage of labour the cervix is. It is important that you continue to feel the baby moving energetically. Once these tests are completed, induction can start. When the hospital is busy, it is not always possible to induce at exactly 41 weeks. You might have to wait, for example, for 41 + 2. But should the baby be moving less than usual, or your amniotic fluid levels are insufficient, or the CTG is not optimal, immediate action will be taken. In these cases you may not always be given the opportunity to be induced at the hospital of your choice. You will then be referred to another hospital in the area.
Induces labour date
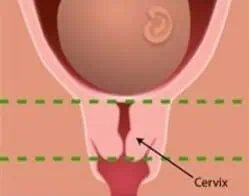
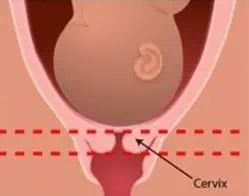
On the day of inducement an internal exam and cardiotocography (CTG) are carried out. Inducement is only possible when the cervix is soft and a little open. An immature cervix is long and stiff. We call this an unripe cervix. There is no access. A mature cervix is shorter. This is called a ripe cervix. It also feels softer and is often already dilated. If the latter is the case, then an induced labour is possible.
When the cervix is unripe, your gynaecologist can make your cervix “mature”. In medical terms this is called “priming”. There are several ways to prime a labour. The obstetrician will discuss which method is best for you. With a very immature cervix it is often necessary to repeat the priming process, sometimes over a few days. You will remain in hospital until you give birth. This happens more commonly to women who are experiencing their first ever labour. When priming, you will often develop a painfully hard stomach which is not classed as a contraction. Only when your cervix is fully ripe, can the gynaecologist induce your labour.
Induced labour begins with the stripping of the membranes along the cervix wall. You will then receive an intravenous drip with contraction triggering medications. Sometimes labour will begin spontaneously upon the stripping of membranes, in which case you will not need medication. The dosage of these contraction inducing drugs will be gradually increased. Many women experience ‘chemical’ contractions as more intense and painful than “natural” contractions. The number and strength of these contractions are recorded via a band wrapped around your belly. Your baby’s condition is continuously assessed using a CTG. This can be done via the belt around your abdomen, or via an electrode placed on your baby’s head.
Usually, a clinical midwife or a doctor’s assistant working under the supervision of the gynaecologist will be present during your labour. They are assisted by a nurse from the labour ward. Students or medical interns may also be present and, if necessary, the gynaecologist on duty at the time. This will mean that we will not be there. In an uncomplicated labour you can often return home within hours.